When Is Formal Disclosure Safe? A Clinical Framework for Betrayal Trauma Recovery
Apr 12, 2026THE TIMING OF TRUTH
Toward Agreed-Upon Criteria for Safe Formal Disclosure in Betrayal Trauma Recovery
A Clinical Framework for CSAT, CPTT, and APSATS Practitioners
By Charlene Lewis, LCSW, CAP, CSAT CST, and Joshua Lewis CRSS
Abstract
Formal Disclosure (FD) is widely recognized as a pivotal intervention in the treatment of sexual betrayal and addiction-related relational trauma. Yet despite its clinical centrality, the field lacks a shared, operationalized framework for determining when FD is safe, for whom, and under what relational conditions it should proceed. This article integrates perspectives from Certified Sex Addiction Therapists (CSATs), Certified Partner Trauma Therapists (CPTTs), and APSATS-credentialed clinicians to propose a multi-domain readiness framework — one that addresses not only the addict's sobriety and accountability, but also the partner's neurological, relational, and psychological capacity to receive disclosure in a way that serves genuine healing. Critically, this article argues that the partner's window of tolerance for truth is a legitimate and clinically necessary focus of pre-disclosure preparation. A partner who cannot yet receive disclosure will not be healed by it — she will be further harmed by it. This is not a character assessment; it is a clinical observation about what trauma does to the nervous system and to relational capacity. Agreed-upon criteria and rough timeframes are proposed, with the understanding that healing is non-linear and clinical judgment must always supersede rigid timelines.
I. Introduction: The Double Bind of Disclosure
Betrayed partners occupy one of the most psychologically agonizing positions in clinical work: they have been systematically deceived by the person they trusted most, and they are now asked to wait — to allow process, to tolerate ambiguity — while their nervous system screams that not knowing is intolerable. This is not a perception problem. It is a neurobiological fact.
Research consistently confirms that the prolonged period between discovery and full disclosure is rated by betrayed partners as one of the most distressing phases of the entire recovery arc, often comparable in distress to the discovery itself (Schneider, Corley, & Irons, 1998). The uncertainty is not merely uncomfortable — it sustains the threat response, prevents nervous system regulation, and makes coherent decision-making about one's own life nearly impossible.
At the same time, the field has accumulated considerable evidence that premature, poorly structured, or clinically unsupported disclosure can catastrophically retraumatize both partners, deepen shame in the addict, and derail the recovery process for months or years (Corley & Schneider, 2002; Steffens & Rennie, 2006). The "trickle truth" pattern — in which the addict discloses partially, then again, then again — is now well-established as among the most damaging disclosure experiences a partner can have.
The clinical imperative, then, is not whether to do Formal Disclosure. The field has reached substantial consensus that FD, done well and within appropriate clinical scaffolding, is beneficial for both partners and for the recovery system as a whole (Drake & Caudill, 2019; Manning, 2015). The imperative is when, how, and with what preparation on both sides of the disclosure table.
This article addresses a question the field has largely left to individual clinical discretion: What are the agreed-upon criteria that make Formal Disclosure safe enough to proceed? And critically — should the partner's own relational and psychological patterns be part of that calculus?
II. The Current Landscape: Three Clinical Traditions
The field of betrayal trauma treatment has developed several distinct but overlapping credentialing traditions, each with its own philosophical emphasis and clinical training approach. Meaningful progress toward shared disclosure criteria requires that we understand — and honestly confront — where these traditions converge and where they differ.
CSATs and the IITAP Model
Certified Sex Addiction Therapists, credentialed through the International Institute for Trauma and Addiction Professionals (IITAP), are trained in the Carnes model of sexual addiction and its treatment. CSAT training includes substantial emphasis on the Formal Disclosure process, including preparation of the disclosure document, management of the disclosure session, and post-disclosure follow-up. The CSAT framework tends to treat FD as a couple-system intervention — the addict writes the disclosure document with clinical support, and both partners engage with it in a structured therapeutic container (Drake & Caudill, 2019).
The CSAT model has historically emphasized the addict's sobriety stability and accountability orientation as primary readiness indicators, while recognizing that the partner's stabilization is also necessary for the process to be productive. More recently, CSAT training has deepened its emphasis on trauma-informed partner care, including recognition that the partner's nervous system state at the time of disclosure significantly affects outcomes.
CPTTs and the Partner-Centered Frame
The Certified Partner Trauma Therapist designation, also offered through IITAP since 2019, represents the field's formal acknowledgment that betrayed partners require specialized clinical attention — not as adjuncts to the addict's recovery, but as primary clients with their own trauma trajectories. As noted in the CPTT framework, partners of sex addicts commonly feel sidelined in a process that tends to allocate clinical resources toward the person with the addiction (IITAP, 2019).
CPTTs bring a specifically partner-centered lens to FD preparation: What does this partner need to actually receive this information? What nervous system state will she be in? What attachment wounds and relational patterns does she bring to the room? This lens is not about protecting the addict from accountability — it is about ensuring that the partner's experience of disclosure serves her healing rather than simply adding another traumatic event to her history.
APSATS and the Multidimensional Partner Trauma Model
The Association of Partners of Sex Addicts Trauma Specialists developed the Multidimensional Partner Trauma Model (MPTM), adapted from Judith Herman's three-phase trauma resolution model (Stabilization, Remembrance and Mourning, Reconnection). APSATS represents perhaps the field's most explicit articulation that partner responses to betrayal are trauma responses — not codependency, not character pathology, not dysfunction — but predictable physiological and psychological reactions to a genuine traumatic stressor.
"The partner of a sex addict has responses that serve as reactions to a stressor that is traumatic in nature, in predictable emotional, behavioral, and physiological ways. She seeks what she cannot find: safety in an unsafe situation."
— Dr. Barbara Steffens, APSATS Founding President
The APSATS framework's emphasis on stabilization as a prerequisite to deeper processing has profound implications for FD timing. Within the MPTM, a partner who has not achieved sufficient stabilization — who remains in the acute phase of traumatic stress — is not clinically prepared to engage with disclosure material in a way that can be integrated. The information may arrive, but it cannot land.
III. The Urgency Problem: Why Waiting Harms and Rushing Harms
The central tension in FD timing is genuine: both urgency and delay carry real clinical risks. Understanding this tension in neurobiological terms, rather than simply relational ones, helps clinicians hold the complexity without defaulting to either extreme.
The Cost of Delay
What remains unknown does not simply create discomfort — it keeps the nervous system in a sustained threat response. When a betrayed partner does not know the extent of what has occurred, her threat-detection system has no object on which to calibrate. She cannot assess actual danger because she does not know what the actual danger is or was. This produces a hypervigilant, scanning state that is biologically exhausting and psychologically destabilizing.
Research conducted through APSATS examining partners' distress levels across different phases of recovery found that the period of uncertainty between discovery and full disclosure consistently ranked among the most painful experiences in the entire recovery arc — often rated more distressing than the disclosure session itself (APSATS Survey Data, cited in Insights Counseling Center, 2025). This is a finding of profound clinical significance: the thing partners and sometimes clinicians dread most — the actual disclosure — is less traumatic than the state of not knowing.
Dr. Carol Juergensen Sheets, LCSW, CCPS, CSAT and APSATS Board Member, captures this neurobiological reality directly:
"That's why I want to protect that brain, because the brain is something you need to make better decisions. It eventually goes back online, but if you overload it, it will take a lot longer, and I'm here to protect you. You've already been betrayed, and you cannot betray yourself by overloading your brain with information you don't want to know. So, in retrospect, you don't want details without having a formal structure to give you the details."
— Carol Juergensen Sheets, LCSW, CCPS, CSAT, APSATS Board Member
The implicit argument here is not that delay is acceptable — it is that structure is essential, and structure takes time to build. Delay without productive preparation is harmful. Delay that constitutes active preparation is clinically necessary.
The Cost of Premature Disclosure
When disclosure occurs before adequate preparation — before the addict has achieved even a minimal sobriety window, before the partner's nervous system has sufficient regulatory capacity, before a clinical container has been established — the outcomes are documented and predictable.
The partner may enter a state of acute traumatic flooding during the session, making it impossible to process or integrate what she is hearing. She may ask for graphic detail that, in the heat of the moment, feels necessary but that will later become intrusive imagery compounding her PTSD symptomatology. The addict, facing what feels like a prosecutorial rather than a witnessing presence, may minimize, omit, or shut down — producing an incomplete disclosure that will ultimately function as yet another installment of trickle truth. And both partners will leave the room without the clinical support structures that transform disclosure from a traumatic event into a therapeutic turning point.
Michelle Mays, LPC, CSAT-S and founder of the Center for Relational Recovery, articulates this clearly:
"Disclosure balances on a razor's edge. When done well, it has the potential to be a critical pivot point for recovering couples, moving them out of the devastation phase that follows discovery of sexual betrayal and into the deep repair and healing of the relationship. When done poorly it has the potential to cause relational trauma and further rupture or damage trust and safety in the relationship."
— Michelle Mays, LPC, CSAT-S
IV. The Partner's Window of Tolerance for Truth
Perhaps the most clinically sensitive — and most underaddressed — dimension of FD readiness is this: the partner's neurological, relational, and psychological state at the time of disclosure is not peripheral to the process. It is constitutive of it. The central clinical question is not simply whether the partner wants disclosure. It is whether she has sufficient capacity to receive it — to take it in, to process it, to use it in service of her own healing and her own decisions.
This distinction matters enormously. A partner who cannot yet receive disclosure will not be healed by it. She will be further harmed by it. That is not a character assessment. It is a clinical observation about what trauma does to the nervous system — and about what the nervous system, in an unregulated state, can and cannot do with information of this magnitude.
The field has, understandably, been cautious about raising this dimension. For decades, betrayed partners were pathologized through the lens of co-addiction — their responses to their partner's betrayal were treated as evidence of their own dysfunction rather than as predictable trauma reactions. The corrective to this injustice, rightly championed by APSATS, has been to firmly center the partner's trauma and resist any framing that introduces even implicit blame. That corrective was necessary and remains important.
But there is a clinical blind spot that can develop in its wake: the assumption that because the partner's pain is real and legitimate, her psychological state is therefore irrelevant to the question of whether disclosure can be received in a way that serves healing. These are separable claims. Her pain is unequivocally legitimate. And simultaneously, her window of tolerance — her current capacity to receive truth without flooding — is a clinically significant variable that determines whether disclosure achieves its therapeutic purpose.
What Trauma Does to the Receiving Capacity
Betrayal trauma is not a single event — it is a sustained assault on the partner's nervous system, her attachment system, and her sense of reality. Research confirms that intimate partner betrayal trauma produces some of the most severe presentations in the PTSD literature, including hypervigilance, intrusive re-experiencing, emotional dysregulation, and dissociation (Steffens & Rennie, 2006). A 2024 study published in Heliyon found that partner betrayal trauma significantly amplifies both anxious and avoidant attachment patterns and markedly decreases self-esteem — creating conditions in which the partner's relational behavior becomes increasingly organized around threat management rather than receptive engagement (Heliyon, 2024).
What this means practically is that the betrayal itself produces, in many partners, precisely the nervous system state that makes receiving disclosure most difficult. This is not the partner's failure. It is trauma's logic. The same hypervigilant scanning that kept her safe while living inside deception becomes, in the disclosure room, a barrier to integration. She may hear the words and be unable to encode them. She may be so flooded that the information bypasses the processing centers of the brain entirely — arriving as raw sensation rather than coherent narrative.
Clinicians will recognize these presentations not as resistance, manipulation, or character pathology, but as the predictable sequelae of sustained relational trauma. Specific presentations that signal a narrowed window of tolerance include:
- The partner whose hypervigilance has organized itself into relentless interrogation — asking the same questions repeatedly not because she hasn't heard the answers, but because her threat system cannot register them as safe
- The partner whose grief has calcified into contempt — not because she is punitive by nature, but because contempt is what rage looks like when it has nowhere else to go
- The partner whose terror of further deception means every answer the addict gives feels like a new lie, regardless of its content — because her trust system has been so thoroughly dismantled that verification itself feels impossible
- The partner who is so neurologically flooded during the disclosure session that she literally cannot encode what she is hearing — who will leave the room and remember almost nothing, not from avoidance, but from dissociation
None of these presentations are reasons to deny the partner disclosure. They are clinical indicators that more preparation is needed — specifically, preparation aimed at widening her window of tolerance enough that the disclosure can actually land rather than simply pass through.
The Systemic Dimension: Why Both Partners' States Matter
There is a second dimension to the partner's receiving capacity that the field has been even more reluctant to name: when the partner enters the disclosure room in a state of extreme dysregulation, the addict's own shame system is directly affected — and this affects the quality and completeness of what is disclosed.
Addiction specialist Patrick Carnes has observed that when the addict perceives the disclosure environment as prosecutorial rather than witnessing, the quality and completeness of disclosure degrades. The shame system — already a central organizing feature of the addiction cycle — interprets the intensity of the partner's dysregulation as confirmation that full truth will result in punishment, and the self-protective response is to minimize, omit, or shut down (Carnes, 2012).
The cruel systemic irony is this: the partner's most activated protective response — the interrogating, demanding, flooding mode that trauma produces — is precisely the response most likely to generate an incomplete disclosure that will retraumatize her further. She needs the truth to heal. Her nervous system, in its most dysregulated state, creates conditions that make it harder for the truth to arrive whole.
This is not the partner's fault. It is the system's logic. And it is a clinical argument — not a moral one — for taking partner preparation as seriously as addict preparation.
The Frame That Serves the Partner
The clinical challenge is to hold this dimension honestly without allowing it to become another instrument of harm against someone who has already been harmed enough. The frame must never be: 'you are too difficult for disclosure to proceed' or 'your anger is the problem.' Those framings would be clinically irresponsible and would replicate the very shaming dynamics that produced her wound.
The frame that serves her — and that all three clinical traditions can endorse — is this:
"Readiness is not about managing the addict's shame. It is about ensuring the partner's healing is served. We want this disclosure to work for you. We want the information to actually land — to be absorbed, integrated, and used in service of your decisions and your life. That requires that enough of you can be present to receive it. The preparation we are doing together is for you."
This reframe is both clinically accurate and irrefutable. No APSATS clinician, no CPTT, no CSAT can reasonably argue that a partner should receive disclosure before she has sufficient capacity to integrate it. The disagreement about framing dissolves entirely when the frame is squarely and unambiguously centered on her healing.
In practical terms, widening the partner's window of tolerance before disclosure involves nervous system stabilization work, psychoeducation about what disclosure is and what it cannot do, the development of pre-formulated questions with her therapist, peer connection with other partners who have moved through this process, and enough individual therapeutic work that her protector parts have been introduced — not eliminated, not shamed — but given enough information that they can, however tentatively, step back for the duration of the session. The goal is not a composed partner. It is a partner who is present enough to receive what she came for.
V. Toward Agreed-Upon Readiness Criteria
What follows is a proposed multi-domain readiness framework, drawing on the combined clinical wisdom of CSAT, CPTT, and APSATS traditions. These criteria are intended as assessment anchors, not rigid checklists. Clinical judgment, grounded in thorough knowledge of each client, must always guide the ultimate determination.
Domain 1: Structural Prerequisites
These are the non-negotiable conditions that must be in place before any clinical readiness assessment begins:
Structural Prerequisites (Non-Negotiable)
- Both partners are working with credentialed specialists: ideally a CSAT for the addict and a CPTT or APSATS-trained clinician for the partner
- A two-therapist model is in place, or the single clinician has established clear protocols for dual-party care with consultation
- No active physical danger, acute suicidality in either partner, or unaddressed legal liability in the disclosure content
- The addict has disclosed no new behaviors in the pre-disclosure preparation period that have not been surfaced to both therapists
- No active divorce or legal separation proceedings (which change the evidentiary implications of disclosure content)
Domain 2: Addict Readiness Criteria
Seminal research by Schneider and Corley (2002) established that addict readiness for disclosure includes both behavioral and psychological dimensions. More recent clinical frameworks have refined these into assessable criteria:
Addict Readiness Indicators
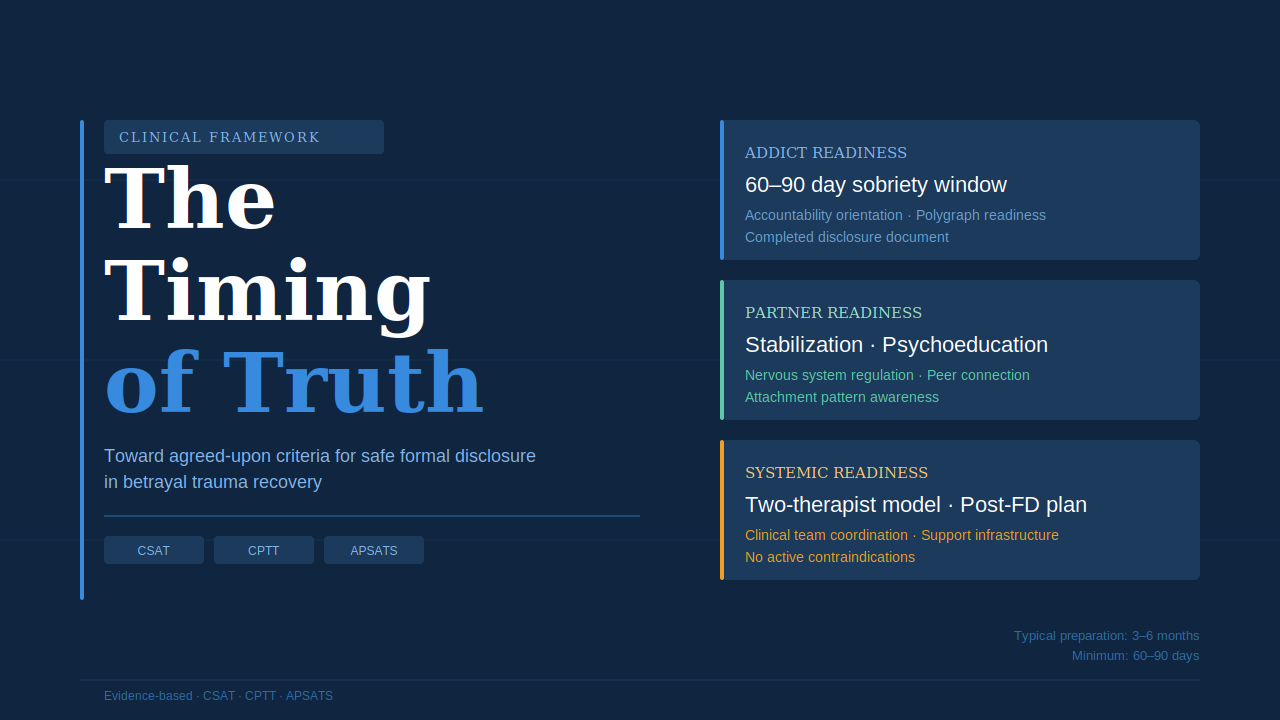
- Minimum sobriety/behavioral stability window: typically 60–90 days of verified behavioral sobriety, with no active acting-out patterns. Some frameworks require 90+ days for more complex presentations
- Genuine accountability orientation: a demonstrable shift from shame-based minimization to accountability-based transparency, visible in therapeutic work over multiple sessions
- Empathy development: some capacity to hold the partner's pain without using it as a trigger for defensive shutdown or counter-attack
- Disclosure document completion: a thorough written disclosure prepared over multiple drafts with CSAT feedback, achieving appropriate scope (not graphic, not vague)
- Polygraph readiness: willingness to support the disclosure with a polygraph examination, either preceding or immediately following, to provide the partner an evidence base for trust
- Inner circle and safety plan: a written commitment to immediate (24–72 hour) disclosure of any future slips or urges
Domain 3: Partner Readiness Criteria
This domain represents the area of greatest clinical underdevelopment in the current literature and the area requiring the most careful clinical attention. Partner readiness is not a fixed threshold — it is a clinical judgment about whether the partner's window of tolerance is wide enough to receive disclosure in a way that can be integrated rather than simply endured.
Partner Readiness Indicators
- Minimum stabilization period: typically 60–90 days of active individual therapeutic work, with evidence of some nervous system regulation capacity (not crisis-free, but able to return to a regulated state)
- Psychoeducation completion: the partner has received education on the disclosure process — what it is, what to expect, what its purpose is, and what it cannot do — sufficient to have an informed, considered relationship to it
- Window of tolerance assessment: the partner demonstrates some capacity to receive difficult information without complete neurological flooding — not composure, but sufficient regulation to encode and process what she hears. Her individual therapist has assessed this directly
- Support infrastructure: a trusted support person is identified and available for the day of and days following disclosure
- Voluntary and considered consent: the partner has arrived at the decision to proceed with FD from a considered, regulated place — not from acute crisis or coercive pressure from the addict or anyone else
- Question formulation: the partner has developed her disclosure questions in advance, in writing, with clinical support — rather than planning to interrogate spontaneously during the session
Domain 4: Systemic and Relational Readiness
Because disclosure occurs in a relational system, the readiness of the system itself is a legitimate clinical consideration:
Systemic Readiness Indicators
- The couple's therapy team has collaborated: the addict's therapist and partner's therapist have communicated, reviewed the disclosure document, and agreed that timing is appropriate
- A post-disclosure support plan is in place for both partners: separate arrangements for the evening and night following disclosure, crisis numbers, and a plan for the next 72 hours
- The relational dynamic does not present acute systemic risk: neither partner is in a position of such extreme activation that the disclosure session is more likely to rupture than to repair
VI. Rough Timeframes: A Proposed Clinical Guideline
One of the most frequently asked questions from clinicians working in this space — and one the field has largely declined to answer directly — is: how long does this preparation realistically take? The following framework represents a clinical synthesis, intended as a guide rather than a mandate.
Minimum Preparation Period: 60–90 Days Post-Discovery
For most presentations, a minimum of 60–90 days of active clinical work on both sides is required before Formal Disclosure can be considered. This is not an arbitrary number. It reflects the minimum time needed for the addict to establish a credible sobriety window, for the partner's acute crisis response to move into a somewhat more regulated phase, and for both therapists to have built sufficient therapeutic alliance and clinical knowledge to assess readiness meaningfully.
This timeframe assumes consistent engagement: weekly individual sessions for both partners, active engagement with the disclosure document preparation, and clinical communication between the treatment team members. Partners who enter treatment with significant prior trauma histories, complex attachment presentations, or who are also managing major life stressors (young children, professional crises, health challenges) may require considerably longer.
Typical Preparation Period: 3–6 Months
In clinical practice, most well-resourced disclosure processes unfold over three to six months of preparation. This timeframe allows for the addict's completion of multiple disclosure document drafts with clinical review, for the partner's psychoeducation and pre-disclosure therapeutic work to reach meaningful depth, and for both therapists to feel confident that the session will produce integration rather than additional fragmentation.
Dr. Jill Manning's clinical guidelines note that because many partners experience trauma in the wake of discovery and partial disclosures, it is important to "reset this experience in a healthy, thorough, and supportive manner and to put all of the information on the table in one place and at one time" — a process that requires careful, unhurried preparation (Manning, 2015).
Complex Presentations: 6–18 Months or More
For presentations involving complex PTSD in the partner, personality disorder features in either partner, prior staggered disclosures that have significantly deepened mistrust, or significant disagreement about the value or desirability of FD, the preparation period may extend considerably. In these cases, the clinical team should consider whether FD in its traditional form is the appropriate intervention, or whether modified approaches — structured partial disclosures, disclosure to the partner's therapist only in an initial phase, or other adaptations — better serve the clinical reality.
The DST model developed by Dr. Omar Minwalla reminds us that for partners who have experienced sustained deceptive sexuality — not a single affair but a chronic system of covert control — the relational trauma is layered and complex, often involving what Minwalla terms Complex Trauma Shaping: the gradual reshaping of the partner's psyche through long-term exposure to a reality that was never what it appeared to be (Minwalla, 2019). These partners may need significantly longer preparation to develop sufficient Self-energy to be present in a disclosure room.
Contraindications Requiring Suspension of FD Planning
Certain clinical presentations require that FD planning be suspended until the contraindication is resolved:
Contraindications (FD Should Not Proceed)
- Active suicidality or recent self-harm in either partner
- Active untreated substance use in either partner
- Domestic violence or intimidation dynamics in the relationship
- Addict currently in active behavioral relapse with no accountability
- Partner in acute traumatic crisis (e.g., recent additional discovery, severe mental health episode)
- Legal proceedings where disclosure content creates direct evidentiary risk
- Addict categorically refusing polygraph support where partner has clearly stated this is essential to her participation
VII. Peer Connection and Witnessed Vulnerability: A Cross-Tradition Consensus
Among the most consistent — and most clinically underutilized — elements of pre-disclosure preparation is the one that all three professional traditions agree upon without reservation: betrayed partners must not be alone. Not in the informal sense of having people around them, but in the clinical sense of having access to other women who understand from the inside what they are living through. The research support for this is substantial, the theoretical grounding is deep, and the cross-tradition consensus is genuine.
The Research Foundation: Social Support as a Buffer Against PTSD
A landmark 2021 meta-analysis by Tirone, Orlowska, Lofgreen, Blais, Stevens, Klassen, Held, and Zalta, published in the European Journal of Psychotraumatology, examined 29 studies assessing the relationship between social support and PTSD symptom severity in 6,510 adult betrayal trauma survivors. The findings are directly clinically relevant: social support functioned as a significant protective factor against PTSD symptoms, with effect sizes that were stronger specifically when the trauma was perpetrated by a romantic partner compared to other perpetrators. The study also found that general positive social support — the kind provided by a community of understanding peers — was associated with meaningfully fewer PTSD symptoms (Tirone et al., 2021).
A companion large-scale meta-analysis by Zalta and colleagues (2021), published in Psychological Bulletin, synthesized 139 studies with 145 independent cross-sectional effect sizes representing 62,803 individuals, and found a near-medium overall effect size (r = -.27) between social support and PTSD severity — consistent across both cross-sectional and longitudinal analyses. The effect was particularly robust for interpersonal trauma populations, as compared to natural disaster survivors, underscoring that the type of support matters most when the source of harm was another person (Zalta et al., 2021).
A third study, by Hahn and colleagues (2021), examined the specific relationship between social support, emotion regulation, and PTSD symptom severity in betrayal versus non-betrayal trauma survivors. The findings yielded a critical clinical implication: for high betrayal trauma survivors specifically, group-based interventions that involve the survivor alongside people with shared experience may be particularly beneficial in enhancing emotion regulation and decreasing PTSD symptomatology (Hahn et al., 2021). The mechanism is not simply comfort — it is the enhancement of regulatory capacity through relational contact.
This last finding carries special weight in the context of disclosure preparation. Emotion regulation is precisely what a partner needs to receive disclosure without flooding. The research suggests that peer connection is not merely supportive — it is one of the primary mechanisms through which that regulatory capacity is built.
Herman's Foundation: The Group as Antidote to Isolation
The theoretical case for peer connection in betrayal trauma recovery does not begin with the social support literature — it begins with Judith Herman's foundational formulation of trauma itself. Herman's three-stage model, which serves as the backbone of the APSATS Multidimensional Partner Trauma Model, was explicit and unambiguous about the role of community in recovery:
"Traumatic events destroy the sustaining bonds between individual and community. Those who have survived learn that their sense of self, of worth, of humanity, depends upon a feeling of connection with others. The solidarity of a group provides the strongest protection against terror and despair, and the strongest antidote to traumatic experience. Trauma isolates; the group re-creates a sense of belonging. Trauma shames and stigmatizes; the group bears witness and affirms. Trauma degrades the victim; the group exalts her. Trauma dehumanizes the victim; the group restores her humanity."
— Judith Lewis Herman, Trauma and Recovery (1992)
Herman further articulated that recovery cannot occur in isolation — that the relational capacities destroyed by trauma can only be rebuilt in relationship: "Recovery can take place only within the context of relationships; it cannot occur in isolation. In her renewed connection with other people, the survivor re-creates the psychological facilities that were damaged or deformed by the traumatic experience" (Herman, 1992). These include the basic operations of trust, autonomy, initiative, competence, identity, and intimacy — the very capacities most systematically undermined by intimate betrayal.
Herman also made specific note of the particular power of homogeneous, time-limited, goal-directed groups for trauma survivors — groups in which members share the same kind of wound. These groups, she observed, offer validation, community, and shared hope in ways that heterogeneous support cannot fully replicate. The partner who sits with other partners who have lived her experience does not need to explain herself, justify her reactions, or translate her pain into language others can understand. The understanding is already there.
Yalom's Therapeutic Factors: Why Witnessing Others Heals
The group therapy literature provides a second theoretical pillar for understanding why peer connection and witnessed vulnerability are not merely supportive adjuncts but active mechanisms of therapeutic change. Irving Yalom's eleven therapeutic factors — developed through decades of group therapy research and clinical observation — identify the specific elements through which group participation produces healing. Several of these factors are directly applicable to the betrayal trauma context:
- Universality: The realization that one is not alone in one's distress — that others share the same thoughts, feelings, and experiences — alleviates the isolation that betrayal specifically produces. As Yalom observed, many individuals suffer with their pain in silence, feeling uniquely alone and uniquely ashamed. Contact with others who share the wound breaks this illusion fundamentally and immediately.
- Instillation of Hope: Observing another woman who was once where you are now — shattered, disoriented, barely functioning — and who is now further along in recovery installs possibility in the nervous system before the individual can generate it from within. Yalom identified this as the most important therapeutic factor, particularly in early stages. In betrayal trauma work, where the partner often cannot imagine healing, witnessed recovery is not motivational — it is therapeutic.
- Imitative Behavior (Vicarious Learning): Group members observe how others handle difficult emotions, speak about painful material, or respond to overwhelming information — and incorporate elements of those approaches into their own experience. The partner who watches another woman speak about her protector parts with curiosity rather than shame is receiving a model she could not generate from her own internal resources.
- Corrective Family Recapitulation: For partners whose early attachment history included critical, shaming, or emotionally unavailable caregivers — which research indicates is common in populations where adult betrayal trauma is present — the experience of being witnessed without judgment by a group of peers provides a corrective relational experience that reorganizes the internal working model of what relationships can be.
- Cohesion and Catharsis: The group creates a container safe enough for emotional release — the kind of grief, rage, and despair that cannot always be expressed in the context of individual therapy without the partner feeling she is burdening her therapist. In a peer community where these feelings are normalized and shared, they can move through rather than accumulate.
Yalom was clear that these factors do not operate independently — they are, in his phrase, intricately interwoven. The presence of strong cohesion enables universality. Universality enables catharsis. Catharsis enables the interpersonal learning that changes how the partner relates to herself and others. What appears to be simple support is, in clinical terms, a complex therapeutic process.
Witnessed Vulnerability: A Mechanism Beyond Support
There is a dimension of peer connection in the betrayal trauma context that goes beyond what the social support literature fully captures, and it is perhaps the most clinically important one: the experience of witnessing another person's authentic vulnerability in real time.
This is distinct from hearing a polished survivor testimonial. When a betrayed partner witnesses another woman — one who is genuinely in the middle of her own healing process — speak honestly about her fear, her rage, her grief, her confusion, her protector parts, and her tentative movement toward integration, something happens in the viewer that mere information transfer cannot produce. The viewer's nervous system tracks, resonates, and co-regulates with what she is witnessing. In the language of interpersonal neurobiology and polyvagal theory, the ventral vagal system — the social engagement system — becomes engaged. The viewer does not simply learn about healing. She begins, physiologically, to experience the possibility of it.
This mechanism is what makes resources like Mari Lee and Sherry Gaba's Facing Heartbreak — a program built around the authentic, recorded therapeutic work of women processing betrayal trauma together — clinically distinct from informational content. The viewer is not watching a presentation about what betrayal trauma is. She is witnessing actual vulnerability, actual processing, actual movement. And that witnessing, when held within an appropriate clinical container, produces what Yalom called a corrective emotional experience: an encounter with something genuinely new that begins to reorganize the internal relational world.
Herman herself captured this dynamic in a striking passage from Trauma and Recovery: "Repeatedly in the testimony of survivors there comes a moment when a sense of connection is restored by another person's unaffected display of generosity. Something in herself that the victim believes to be irretrievably destroyed — faith, decency, courage — is reawakened by an example of common altruism. Mirrored in the actions of others, the survivor recognizes and reclaims a lost part of herself" (Herman, 1992).
This is witnessed vulnerability at work. And it is not a supplement to clinical treatment — it is one of the mechanisms through which healing becomes possible.
Where All Three Traditions Converge
The cross-tradition consensus on peer connection and witnessed experience is among the clearest in this entire clinical landscape. Each tradition grounds its endorsement in its own theoretical framework, and the convergence is genuine rather than forced:
APSATS grounds it in Herman's trauma model and the MPTM's explicit emphasis on Phase 1 stabilization through connection and Phase 3 reconnection as a therapeutic goal. The APSATS framework has always recognized that the partner's isolation is itself a wound inflicted by the addict's system of secrecy — and that healing that wound requires being genuinely witnessed by others who understand. Peer community is not supplementary to APSATS-informed treatment; it is structurally embedded in the model's three phases.
CSATs ground it in the Carnes-informed recognition that witnessed experience and peer community are among the most powerful forces in addiction recovery — for addicts and partners alike. The same mechanism that makes twelve-step programs effective — identification, universality, instillation of hope, vicarious learning — operates in peer communities for betrayed partners. Carnes himself observed that isolated shame is the fuel of addiction's cycle; the antidote for both the addict and the partner is authentic community (Carnes, 2012).
CPTTs ground it in attachment theory: secure connection with safe others is the primary mechanism through which a dysregulated attachment system begins to reorganize toward earned security. After betrayal, the partner's attachment system is in crisis — her most trusted bond has proven catastrophically unsafe. Peer connection with women who understand this experience from the inside provides what the addict currently cannot: safe, attentive, non-judgmental relational presence. This begins the slow process of rebuilding the nervous system's evidence that trustworthy attachment exists.
The Clinical Caveat: Scaffolding, Not Substitution
All three traditions would also converge on the one significant caveat: the quality of the clinical container matters enormously. Herman was explicit that not all groups are helpful — successful groups require structure, safety, and skilled facilitation. She cautioned that groups which lack these elements can retraumatize rather than heal. The social support meta-analysis by Tirone and colleagues (2021) was similarly specific: negative social reactions — including blame, dismissiveness, or responses that reinforce shame — were associated with more PTSD symptoms, not fewer. The quality of witnessed experience matters as much as its presence.
This has direct implications for how peer connection and witnessed vulnerability resources are positioned within the clinical arc. A partner in acute traumatic crisis who engages with powerful witnessed vulnerability content without adequate individual clinical support to process what surfaces may experience activation without integration — which can compound rather than relieve symptoms. The content itself is not the risk. Unsupported activation is the risk.
The appropriate clinical frame — one that all three traditions can endorse — is this: peer connection and witnessed vulnerability resources like Facing Heartbreak function as specialized stabilization and psychoeducation tools that run alongside individual therapy, not instead of it. They deliver what individual therapy cannot — witnessed vulnerability, peer normalization, the experience of not being alone in this, the installation of hope through observed recovery — while the individual therapeutic relationship delivers what peer resources cannot: personalized, responsive, crisis-capable clinical support.
This is not a limitation of peer-based and witnessed-experience resources. It is an accurate description of what makes them uniquely valuable — and it is a framing that CSAT, CPTT, and APSATS clinicians can all endorse without reservation.
Positioning Within the Clinical Arc
Given the research and the theoretical consensus, peer connection and witnessed vulnerability resources are of benefit beginning in the earliest stages of stabilization — provided a clinical container is in place to process what surfaces. Concretely:
- In the first weeks post-discovery, even limited peer contact — a support group, a structured online community, or exposure to witnessed-experience content — begins to address the isolation that compounds acute traumatic stress. This aligns with the APSATS Phase 1 (Stabilization) mandate.
- During the pre-disclosure preparation period, peer connection actively builds the relational resources, emotion regulation capacity, and nervous system resilience that the partner will need to receive disclosure. This is not incidental to disclosure readiness — it is constitutive of it.
- In the post-disclosure period, peer support offers something individual therapy cannot provide in the same way: the company of women who have survived what she has just survived. The normalization of post-disclosure grief, disorientation, and destabilization by peers who have lived it accelerates integration and reduces the sense that something has gone wrong.
The clinical recommendation, grounded in research and cross-tradition consensus, is therefore not whether to incorporate peer connection and witnessed experience into the partner's treatment arc — but how to do so with sufficient clinical scaffolding that the activation these resources produce can be metabolized into healing rather than added to the load of unprocessed trauma.
VIII. Psychoeducation as Clinical Preparation
One of the most important — and most underutilized — elements of pre-disclosure preparation is psychoeducation for the partner about what disclosure is, what it is not, and what receiving it will require of her. This education is not incidental to disclosure preparation. It is constitutive of it.
Partners deserve to understand before the session:
- What FD will and will not tell her. FD is not a comprehensive inventory of the addict's subjective experience, motivations, or emotional life. It is a factual accounting of behaviors. It will provide clarity. It will not provide understanding.
- That the goal is informed decision-making, not reconciliation. The purpose of FD is to restore the partner's right to truth and choice — to give her the information she needs to make her own decisions about her life. It is not a tool of relational repair, even if it may contribute to repair in the longer term.
- That she will likely feel worse before she feels better. The integration of disclosure information is not immediate. Most partners experience a resurgence of acute grief and shock in the days following FD. This is not a sign that FD was wrong or that recovery is impossible.
- How to manage her questions. The partner should enter the session with pre-formulated, prioritized questions developed with her therapist. Spontaneous interrogation in the session is likely to produce graphic detail that increases trauma without adding safety.
- That she has the right to call for breaks and to set the pace. FD is not an endurance test. She is permitted to feel, to pause, to return.
The partner's therapist — ideally a CPTT or APSATS-credentialed clinician — plays a central role in this psychoeducational preparation, helping the partner move from reactive urgency ("I need to know everything right now") to informed readiness ("I know what I'm asking for and I'm as prepared as I can be to receive it").
IX. Conclusion: What Everyone Can Reasonably Live With
The field does not need perfect consensus on every nuance of Formal Disclosure practice. What it needs is a workable shared framework that clinicians trained across different credentialing traditions can bring to their clinical work without fundamental contradiction.
The framework proposed in this article attempts to offer exactly that. Its core commitments are:
- FD is clinically necessary and beneficial when done well. The field's consensus on this point is clear and well-supported by research and clinical experience.
- Neither urgency nor avoidance serves the partner's healing. The goal is not speed; it is appropriate preparation that enables the partner to actually receive — not merely survive — the disclosure.
- Both partners require preparation, and both forms of preparation are clinically legitimate. Assessing the partner's window of tolerance for truth — her current neurological and psychological capacity to receive and integrate disclosure — is not about protecting the addict from accountability. It is about ensuring the partner's healing is served. A partner who survives disclosure is not the same as a partner who receives it. The field's ethical obligation is to the latter.
- Peer connection and witnessed vulnerability are not adjuncts to preparation — they are therapeutic mechanisms in their own right. Research across 29 studies of 6,510 betrayal trauma survivors demonstrates that social support is among the most robust protective factors against PTSD symptoms. All three clinical traditions ground their endorsement of peer community in their own theoretical frameworks — APSATS in Herman's three-phase model, CSATs in the peer recovery tradition, CPTTs in attachment theory — and the consensus is genuine. Resources delivering witnessed vulnerability alongside individual therapy build the very regulatory capacity the partner needs to receive disclosure.
- Sixty to ninety days represents a minimum preparation period for most presentations. Most well-resourced disclosures unfold over three to six months. Complex presentations require more.
- Structural prerequisites are non-negotiable. No amount of relational readiness can substitute for the absence of a two-therapist model, a sobriety window, or safety from acute risk.
Ultimately, what disclosure restores to the betrayed partner is something the addiction took from her: truth and choice. As Dan Drake, LMFT, CSAT-S notes, "What sexual betrayal takes from you is choice and truth. The reality you thought you were living turns out to not be the whole truth. A Full Disclosure is a way of getting to a foundation of truth in your relationship" (Drake & Caudill, 2019).
That foundation is worth building carefully. The partner — who has already lost so much — deserves a disclosure that actually serves her healing. The preparation required to make that possible is not an obstacle to her recovery. It is part of it.
References
Association of Partners of Sex Addicts Trauma Specialists (APSATS). (2014). Multidimensional Partner Trauma Model. apsats.org
Carnes, P. J. (2012). Facing the Shadow: Starting Sexual and Relationship Recovery (3rd ed.). Gentle Path Press.
Corley, M. D., & Schneider, J. P. (2002). Disclosing secrets: Guidelines for therapists working with sex addicts and co-addicts. Sexual Addiction & Compulsivity, 9(1–2), 43–67.
Drake, D., & Caudill, J. (2019). Full Disclosure: How to Share the Truth After Sexual Betrayal. Gentle Path Press.
Heliyon (2024). Partner betrayal trauma and trust: Understanding the impact on attachment style and self-esteem. ScienceDirect. https://doi.org/10.1016/j.heliyon.2024
Hahn, C. K., Hahn, A. M., Gaster, S., & Quevillon, R. (2021). Betrayal vs. nonbetrayal trauma: Examining the different effects of social support and emotion regulation on PTSD symptom severity. Psychological Trauma: Theory, Research, Practice, and Policy, 13(7), 802–809.
Herman, J. L. (1992). Trauma and Recovery: The Aftermath of Violence — From Domestic Abuse to Political Terror. Basic Books.
Herman, J. L. (1998). Recovery from psychological trauma. Psychiatry and Clinical Neurosciences, 52(S1), S145–S150.
International Institute for Trauma and Addiction Professionals (IITAP). (2019). Certified Partner Trauma Therapist (CPTT) Program. iitap.com
Manning, J. C. (2015). Recommendations for Therapeutic Disclosures. drjillmanning.com
Mays, M. (2023). The Betrayal Bind: How to Heal When the Person You Love the Most Has Hurt You the Worst. Central Recovery Press.
Mays, M. (2024). Relational Recovery Disclosure Prep Model. relationalrecovery.com
Minwalla, O. (2013). The Diagnostic and Clinical Treatment Formulation for Compulsive-Abusive Sexual-Relational Disorders (CASRD). Institute for Sexual Health.
Minwalla, O. (2019). Deceptive Sexuality and Trauma Treatment (DSTT) Model. theinstituteforsexualhealth.com
Schneider, J. P., Corley, M. D., & Irons, R. (1998). Surviving disclosure of infidelity: Results of an international survey of 164 recovering sex addicts and partners. Sexual Addiction & Compulsivity, 5(3), 189–217.
Schneider, J. P., Corley, M. D., & Irons, R. (2012). Surviving disclosure of sexual betrayal: Information and guidance for betrayed partners. Sexual Addiction & Compulsivity, 19(4), 204–223.
Steffens, B. A., & Rennie, R. L. (2006). The traumatic nature of disclosure for wives of sexual addicts. Sexual Addiction & Compulsivity, 13(2–3), 247–267.
Steffens, B. A., & Means, M. (2009). Your Sexually Addicted Spouse: How Partners Can Cope and Heal. New Harbinger Publications.
Tirone, V., Orlowska, D., Lofgreen, A. M., Blais, R. K., Stevens, N. R., Klassen, B., Held, P., & Zalta, A. K. (2021). The association between social support and posttraumatic stress symptoms among survivors of betrayal trauma: A meta-analysis. European Journal of Psychotraumatology, 12(1), 1883925.
Yalom, I. D., & Leszcz, M. (2005). The Theory and Practice of Group Psychotherapy (5th ed.). Basic Books.
Zalta, A. K., Tirone, V., Orlowska, D., Blais, R. K., Lofgreen, A., Klassen, B., Held, P., Stevens, N. R., Adkins, E., & Dent, A. L. (2021). Examining moderators of the relationship between social support and self-reported PTSD symptoms: A meta-analysis. Psychological Bulletin, 147(1), 33–54.
This article represents a synthesis of current clinical literature and practice wisdom and is intended as a resource for practitioners credentialed in betrayal trauma treatment. It does not constitute formal clinical guidelines from APSATS, IITAP, or any credentialing body. All clinical decisions should be made in consultation with appropriate supervisors and with full attention to individual client presentation and context.
Don't miss a beat!
New moves, motivation, and classes delivered to your inbox.
We hate SPAM. We will never sell your information, for any reason.
Author

